08 9544 5200
Gastric Bypass Surgery
How We Perform Gastric Bypass Surgery
When we do the Gastric Bypass surgery, Roux en-Y, we want to make a very small pouch out of the upper stomach, to restrict the amount of food which can be eaten. That pouch is separated from the rest of the stomach, which is bypassed, by creating a new pathway into the intestines. This pathway is called a “Roux en-Y” (named after the French surgeon, Dr. Roux, who first described this reconstruction in the 1800’s). The bowel is cut, and reconstructed in a Y configuration, so that two parts of the GI tract can feed into one.
Whether we do the gastric bypass surgery through an incision, or laparoscopically, the basic methods, anatomy, and the results are the same, although the instruments differ. Here’s how we do the gastric bypass surgical procedure laparoscopically:
Operating Ports
Laparoscopy is done through “ports”, which are tubes that we pass instruments through, to operate on the internal organs. We place several of these in the abdominal wall, through tiny incisions.
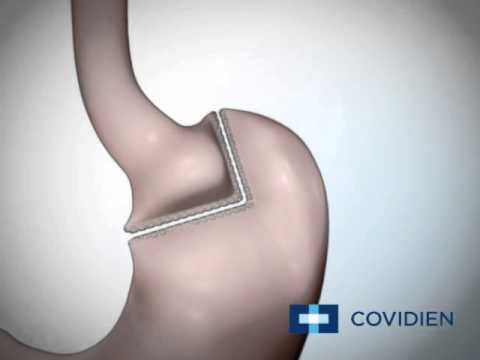
Measuring and Cutting the Stomach for a Gastric Bypass
In a Gastric Bypass we make the upper stomach pouch very small, so that it will hold about 10-15 ml of food. The next stage of the Gastric Bypass is to divide the stomach with a special stapler which makes several rows of staples on each side, and cuts between them. The small upper pouch will be the new stomach. The large lower part of the stomach will no longer contain any food. It still has all its blood vessels, and makes normal secretions, and these can exit through its bottom connection, the pylorus, which is undisturbed.
Constructing the Roux Limb
We cut the small intestine a few inches below the stomach, and measure a length of it, to be used as the “Roux limb”, which will attach to the new little stomach. The bowel is connected side-to-side, to form the ‘Y’. The upper end of the Roux limb is passed behind the large intestine and the bypassed stomach, because that is the most direct and shortest route to the little upper stomach pouch.
Inserting the Stapler Anvil
The stomach pouch is so small, that suturing a connection would be very difficult, especially by a gastric bypass via laparoscopy. We then pass a part of the stapler, “the anvil” through one of the abdominal wall incisions (ports) and insert it through a small cut into the stomach pouch. When the anvil is in place, we bring its stem through the side of the pouch, to connect it to the body of the stapler.
Inserting the Stapler and Connecting
With the anvil in place, we insert the body of the stapler into the abdomen, through one of the small port sites, and then slide it inside the bowel, to make the connection. The stapler and anvil are snapped together, and the stapler is screwed shut, then fired, creating two circles of staples, with a hole through their middle, like a donut, and uniting the stomach pouch to the upper end of the Roux limb.
After the circular stapler is removed, the opened end of the bowel is re-closed with another application of the linear stapler. This completes the construction of the connection between the stomach and small bowel. The main part of the Gastric Bypass surgery is now over.
Note that food enters the tiny stomach pouch, and exits through a small hole into the small intestine, which has been moved up, behind the lower stomach and large intestine, to be connected. The lower, larger stomach pouch no longer receives any food, but still has a blood supply and is able to secrete digestive juices, which can leave by the same route as they always have, through the connection at the lower end (the “pylorus”), to pass down the duodenum, to the Y-connection just a few inches downstream. All the food and digestive juices still travel through about 25 feet of small intestine, where absorption is essentially complete. However, the small size of the stomach pouch may make one feel full quickly, while the food entering the upper small intestine causes a sense of satisfaction and indifference to further eating – the “Who Cares?” feeling.
Testing and Tidying Up
Once all the connections are made, the Gastric Bypass is completed by testing the upper one by inflating the stomach pouch with air from above, and looking for air bubbles while the connection is submerged under rinse water in the abdomen. The abdomen is rinsed out and tidied up, a small drain tube is put in place, the ports are removed, and the operation is over.
All drawings courtesy of Ethicon Endosurgery, Inc.
Advantages of Gastric Bypass Surgery:
- Good operation for sweet eaters*
- Difficult to “cheat” with sweets and chocolates because of
intolerance due to “dumping syndrome”.* - Long track record*
- Tend to lose a little more weight than lap. gastric band*
- More successful then lap band in keeping the weight off
long term* - Quicker improvement with sugar control in diabetics*
Disadvantages of Bypass Surgery:
- Permanent
- Possibility of a staple line leak
- Minor late weight regain 10-20% after 2-5 yrs*
- Nutritional/ mineral supplements required*
Residual stomach capacity post-Gastric Bypass: 10-15 mls*
Estimated weight loss with Gastric Bypass surgery is: 60-70% EWL over 2 years.*
*Results may vary for individual patients. Please consult your surgeon.